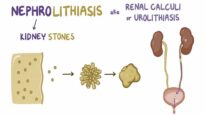
Uric acid stones account for 5 to 10 percent of all kidney stones in the United States and Europe; however, they comprise 40 percent or more of stones in areas with hot, arid climates.
●Pathogenesis
The most important biochemical risk factor for uric acid nephrolithiasis is a persistently low urine pH. Hyperuricosuria is not always present in patients with pure uric acid stones. Low urine volume (with a high urine concentration of uric acid) and an acid urine pH drive the conversion of the relatively soluble urate salt into insoluble uric acid.
●Predisposing clinical conditions
Common clinical conditions that increase the risk of uric acid stone formation include gout, chronic diarrhea, diabetes, and the metabolic syndrome.
●Diagnosis
Patients with uric acid nephrolithiasis usually present with the acute onset of flank pain, often in the setting of a known predisposing condition (such as gout). Non-contrast-enhanced computerized tomography (CT) typically reveals the presence of a stone. Confirmation of the diagnosis is best made by chemical analysis of a stone that has been passed.
●Treatment
Invasive treatments may be needed for large and acutely symptomatic stones. However, for asymptomatic kidney stones, non-invasive treatments should be attempted first since hydration and urinary alkalinization can lead to dissolution of pure uric acid stones.
•For patients with uric acid nephrolithiasis, we recommend urinary alkalinization and an increased fluid intake (Grade 1B).
–Alkalinization is generally performed with potassium citrate or potassium bicarbonate and should target a urine pH between 6.5 and 7.
–Patients with uric acid stones should be encouraged to drink enough fluids to achieve a 24-hour urine volume of at least two liters.
•For patients who continue to form uric acid stones despite urinary alkalinization (or who cannot tolerate supplemental alkali) and a higher fluid intake, we recommend treatment with a xanthine oxidase inhibitor (Grade 1B). Such patients usually have hyperuricosuria (greater than 1000 mg/day [6 mmol/day]), but xanthine oxidase inhibitors are warranted even in patients with recurrent uric acid stones and lower levels of urinary uric acid excretion