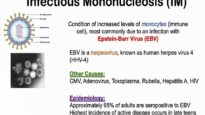
Epidemiology − Infectious mononucleosis (IM) is an acute illness due to Epstein-Barr virus (EBV) infection, which occurs mainly in adolescents and young adults.
●Clinical manifestations − IM is classically characterized by fever, pharyngitis, fatigue, and lymphadenopathy. Other findings can include splenomegaly and palatal petechiae. Cervical lymphadenopathy tends to involve the posterior chain of lymph nodes.
●Complications − Rare complications include splenic rupture and airway obstruction.
●Rash − A generalized maculopapular, urticarial, or petechial rash is occasionally seen. Rash may be more common following the administration of ampicillin or amoxicillin.
●Laboratory abnormalities − Common laboratory findings include an absolute or relative lymphocytosis, an increased proportion of atypical lymphocytes, and elevated aminotransferases.
●Diagnostic evaluation − Patients with suspected IM, based upon the history and physical examination, should have a white blood cell count with differential and a heterophile test (eg, the “Monospot” test) or EBV-specific antibody testing. In addition, patients should also have a diagnostic evaluation for streptococcal infection by culture or antigen testing.
●Role of EBV-specific antibodies − In a patient with a compatible syndrome and a negative heterophile antibody, the Monospot test can be repeated since this test can be negative during the first week of clinical illness. Alternatively (or in addition), EBV-specific antibodies (IgM and IgG antibodies directed against viral capsid antigen [VCA], IgG antibodies to nuclear antigen and early antigen) can be obtained. EBV-specific antibodies can be particularly helpful if the patient has a repeatedly negative Monospot.
●EBV-negative mononucleosis − The presence of IgG antibodies to EBV nuclear antigen (EBNA), or the absence of IgG and IgM antibodies to VCA, excludes acute primary EBV infection and should prompt consideration of alternative etiologies of a mononucleosis-like illness, such as cytomegalovirus (CMV), primary HIV infection, and toxoplasmosis. The most important diagnosis to exclude is primary HIV infection; this can be accomplished with both quantitative HIV RNA and HIV antibody testing. The evaluation for CMV takes on great importance in the pregnant female.
●Treatment − Primary EBV infections rarely require more than supportive therapy.
•In individuals with impending airway obstruction, we suggest corticosteroids, as well as emergent consultation with an otolaryngologist.
●Resuming sports − For athletes planning to resume noncontact sports, training can be gradually restarted three weeks from symptom onset. For strenuous contact sports or activities associated with increased intraabdominal pressure, we suggest waiting for a minimum of four weeks after illness onset