•Patients with peptic ulcer disease should be tested for Helicobacter pylori (H. pylori). Patients with H. pylori should be treated with a goal of eradication of H. pylori infection. In patients treated for H. pylori, eradication of infection should be confirmed four or more weeks after the completion of eradication therapy.
•Patients with peptic ulcers should be advised to avoid nonsteroidal anti-inflammatory drugs (NSAIDs). Contributing factors should be addressed and treated (eg, treating medical comorbidities, poor nutritional status, ischemia).
●Antisecretory therapy
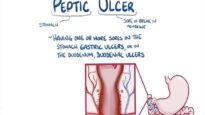
All patients with peptic ulcer disease should receive antisecretory therapy with a proton pump inhibitor (PPI) to facilitate ulcer healing. The choice and duration of therapy varies based on the etiology, ulcer location (eg, gastric or duodenal), and the presence of ulcer complications (eg, bleeding, perforation, penetration, or gastric outlet obstruction).
●Indications for surveillance endoscopy
•Patients with duodenal ulcers who have been treated do not need further endoscopy unless symptoms persist at four weeks or recur.
•In patients with gastric ulcers, the decision to perform surveillance endoscopy should be individualized. We suggest surveillance endoscopy (with biopsies of the ulcer if still present) be performed after 8 to 12 weeks of antisecretory therapy in patients with gastric ulcers and any one of the following:
–Symptoms despite medical therapy
–Unclear etiology
–Giant gastric ulcer (>2 cm)
–Biopsies not performed or inadequate sampling on the index upper endoscopy
–Ulcer appears suspicious for malignancy on index upper endoscopy (mass lesion, elevated irregular ulcer borders, or abnormal adjacent mucosal folds)
–Patients with bleeding ulcers at initial presentation who show signs of continued bleeding









![Appendicitis Signs, Symptoms, Examination, Diagnosis, Treatment [Nursing Medical]](https://mediube.com/wp-content/uploads/2024/09/Appendicitis-Signs-Symptoms-Examination-Diagnosis-Treatment-Nursing-Medical-277x156.png)