Acute pancreatitis is an acute inflammatory process of the pancreas. Acute pancreatitis can be divided into two broad categories: edematous, interstitial acute pancreatitis and necrotizing acute pancreatitis. Mild acute pancreatitis is characterized by the absence of organ failure and local or systemic complications. Moderately severe acute pancreatitis is characterized by no organ failure or transient organ failure (<48 hours) and/or local complications. Severe acute pancreatitis is characterized by persistent organ failure (>48 hours) that may involve one or multiple organs. (See ‘Classification’ above.)
●Initial evaluation
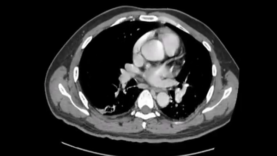
At initial evaluation, the severity of acute pancreatitis should be assessed by clinical examination to assess for early fluid losses, organ failure, and systemic inflammatory response syndrome (SIRS) score. Routine abdominal computed tomography (CT) scan is not recommended at initial presentation in patients with acute pancreatitis unless there is uncertainty about the diagnosis.
●Indication for monitored or intensive care unit
Admission to a monitored or intensive care unit is indicated in patients with severe acute pancreatitis and in patients with acute pancreatitis who meet one or more of the following parameters:
•Pulse <40 or >150 beats/minute
•Systolic arterial pressure <80 mmHg or mean arterial pressure <60 mmHg or diastolic arterial pressure >120 mmHg
Acute pancreatitis is treated with supportive care including pain control, goal-directed intravenous fluids especially during the first 24 hours, and correction of electrolyte and metabolic abnormalities. The majority of patients with mild pancreatitis require no further therapy, and recover within three to seven days. Patients with moderately severe and severe pancreatitis require more intensive monitoring as they have transient (<48 hours) or persistent (>48 hours) organ failure and local or systemic complications.
●Pain control
Abdominal pain is often the predominant symptom in patients with acute pancreatitis. Adequate pain control requires the use of intravenous opiates, such as morphine and fentanyl, usually in the form of a patient-controlled analgesia pump.
●Nutrition
In patients with mild pancreatitis, recovery generally occurs quickly, making it unnecessary to initiate supplemental nutrition. A soft diet can be started early (within 24 hours) as tolerated if the pain is decreasing and inflammatory markers are improving. We usually start with a low-residue, low-fat, and soft diet, provided there is no evidence of ileus or significant nausea and/or vomiting.
In patients with severe pancreatitis, we recommend enteral nutrition through a nasojejunal tube placed endoscopically or radiologically rather than initiating parenteral nutrition (Grade 1B). If the target rate is not achieved within 48 to 72 hours and if severe acute pancreatitis is not resolved, supplemental parenteral nutrition should be provided.
●Indications for follow-up imaging
Patients with moderately severe or severe acute pancreatitis, signs of sepsis, or clinical deterioration 72 hours after initial presentation, should undergo a contrast-enhanced CT scan to assess the presence of pancreatic or extrapancreatic necrosis and local complications. Patients with persistent organ failure and extensive local complications should be transferred to centers of expertise.