During the initial 24 hours, severe acute pancreatitis (AP) can be predicted using clinical, laboratory, and radiologic risk factors, many of which have been incorporated into scoring systems such as the systemic inflammatory response syndrome (SIRS) score, the Acute Physiology and Chronic Health Examination (APACHE) II score, the bedside index of severity in acute pancreatitis score, and the computed tomography (CT) severity index. However, these predictive models have low specificity (ie, high false-positive rates), which, when coupled with the low prevalence of severe AP, result in low positive predictive values. However, of the scoring systems, we favor the SIRS score because it is simple, cheap, readily available, and as accurate as any other complex scoring system, especially persistent SIRS.
Abdominal imaging
•Indication and timing of abdominal CT
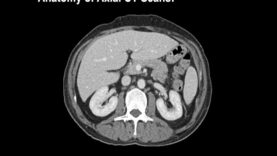
We suggest a contrast-enhanced CT be performed in patients considered to have severe AP based upon clinical criteria or possibly the APACHE II score to determine if necrotizing pancreatitis is present.
A CT scan is not required on the first day unless other diagnoses are being considered. It takes time for pancreatic necrosis to develop and thus CT may be normal in the first 48 to 72 hours. Although there are some data that ionic contrast may worsen pancreatitis, the association is probably not strong, and the information obtained from the CT scan justifies the potential risk.
•Role of MRI
Magnetic resonance imaging is a useful imaging tool in pancreatitis, especially to identify stones in the bile duct, visualize pancreatic duct, and to distinguish the contents of fluid collections seen on CT. However, the limitations in the setting of acute pancreatitis include high cost and need for prolonged examination time.
Predictors of severe disease
Clinical signs and laboratory tests have an adjunctive role in predicting the severity of acute pancreatitis. We agree with the guidelines issued by the American Gastroenterology Association, American College of Gastroenterology, and International Association of Pancreatology/American Pancreatic Association, which suggest that advanced age, comorbidities, body mass index >30, pleural effusion or pulmonary infiltrates, hematocrit >44, blood urea nitrogen (BUN) >20, rising BUN, high creatinine, initial SIRS score ≥2, persistent SIRS, and persistent organ failure are moderately useful as predictors of severe disease.