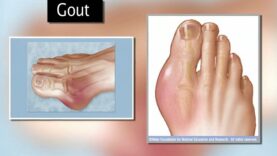
Gout (monosodium urate [MSU] crystal deposition disease) is characterized biochemically by extracellular fluid urate saturation, which is reflected in the blood by hyperuricemia, with serum or plasma urate concentrations exceeding 6.8 mg/dL (approximately 400 micromol/L); this level of urate is the approximate limit of urate solubile The clinical manifestations of gout may include:
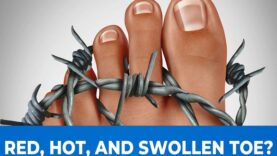
●Recurrent flares of inflammatory arthritis (gout flare)
●A chronic arthropathy
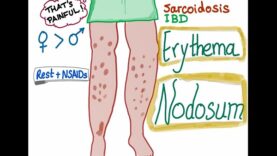
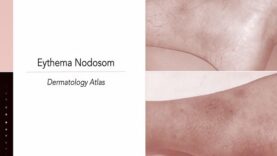
●Accumulation of urate crystals in the form of tophaceous deposits
●Uric acid nephrolithiasis
●A chronic nephropathy that, in gouty patients, is most often due to comorbid states
Hyperuricemia is a necessary but not sufficient precondition for the development of urate crystal deposition disease and should be distinguished from gout, the clinical syndrome. Most hyperuricemic individuals never experience a clinical event resulting from urate crystal deposition.
The clinical manifestations and diagnosis of gout flares, chronic gouty arthritis, and tophaceous disease will be reviewed here.
Topics discussed separately include:
●Mechanisms underlying hyperuricemia and nonmodifiable and modifiable risk factors for hyperuricemia
●Asymptomatic hyperuricemia
●Treatment of gout flares
●Prevention of recurrent gout flares
●Acute and chronic uric acid nephropathy and uric acid nephrolithiasis
●Hyperuricemia and gout in recipients of renal transplants