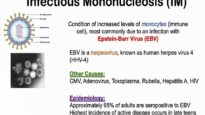
Contact of Epstein-Barr virus (EBV) with oropharyngeal epithelial cells allows replication of the virus, release of EBV into the oropharyngeal secretions, and infection of B cells in the lymphoid-rich areas of the oropharynx. EBV-infected B cells are responsible for the dissemination of infection throughout the lymphoreticular system. The incubation period prior to the development of symptoms averages four to eight weeks.
A prospective study was performed in 20 subjects with serologically confirmed primary EBV infection to assess viral kinetics in various compartments, including whole blood, peripheral blood mononuclear cells, and oral wash fluid. The median half-life of viral elimination from whole blood in 19 subjects was three days; quantity in this compartment correlated with the severity of symptoms. In contrast, virus persisted at an elevated level for 32 weeks in the oropharynx in asymptomatic subjects, consistent with the theory that EBV is transmitted via saliva.
Primary EBV infection of B lymphocytes induces circulating antibodies directed against viral and unrelated antigens found on sheep and horse red cells. The latter antibodies, termed heterophile antibodies, are a heterogeneous group of mostly immunoglobulin (Ig)M antibodies that do not cross-react with EBV antigens. Rarely, infected cells produce antineutrophil, antierythrocyte, and antiplatelet antibodies, which are responsible for some of the less common clinical manifestations associated with IM (see below). An EBV-specific serologic response can also be documented, although this is necessary for less than 10 percent of heterophile antibody-negative IM cases.
EBV-specific cytotoxic T-lymphocytes are considered essential in controlling acute and reactivation infection. T cell activation leads to a T helper 1-type profile with production of interleukin-2 and interferon-gamma cytokines. The atypical lymphocytes that appear in the peripheral blood of patients with acute IM between one and three weeks after the onset of symptoms are primarily activated (HLA-DR+) CD8+ T-cells and also include CD16+ natural killer (NK) cells.
Despite these immune responses, which control the initial lytic infection, EBV becomes a lifelong infection as it establishes latency with periodic reactivation with oral shedding of EBV. On the other hand, insufficient cellular immune responses may result in a poorly-controlled EBV infection and/or generate an EBV-induced malignancy. Even with sufficient immune responses, some epidemiological studies have linked IM to increased risks of other conditions, such as Hodgkin lymphoma and other cancers. Other studies have linked the acquisition of infection to increased risks for autoimmune disorders, such as multiple sclerosis or systemic lupus erythematosus. Such associations will require additional study beyond purely observational studies to prove causation as well as to determine whether they could be a result of direct viral or rather immunological consequences. Such concerns have heightened interest in exploring potential preventative strategies, such as an EBV vaccine