There are numerous causes of ascites, but the most common cause of ascites in the United States is cirrhosis. Other common causes of ascites include malignancy-related ascites and ascites due to heart failure. Approximately 5 percent of patients will have two or even three causes for ascites formation.
●Clinical manifestations
Patients with ascites typically report progressive abdominal distension that may be painless or associated with abdominal discomfort. The time course over which the distension develops depends upon the etiology of the ascites. It may develop over the course of days (eg, bloody ascites due to trauma) or months (eg, malignant ascites). Patients may also complain of weight gain, shortness of breath, early satiety, and dyspnea resulting from fluid accumulation and increased abdominal pressure.
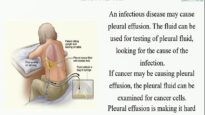
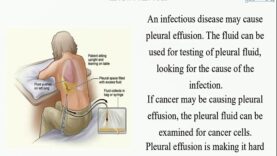
Patients with ascites, regardless of the etiology, will typically have flank dullness on examination. Other findings include shifting dullness (a change in location of dullness to percussion when the patient is turned due to movement of the ascites) and/or evidence of pleural effusions (eg, decreased breath sounds or dullness to percussion). Patients may also have physical examination findings related to the underlying cause of the ascites, such as stigmata of cirrhosis.
●Diagnosis
The diagnosis of ascites is established with a combination of physical examination and abdominal imaging (usually ultrasonography). Once the diagnosis of ascites is made, the next step is to look for the cause. This typically includes a paracentesis to evaluate the ascitic fluid.
●Analyzing ascitic fluid
Abdominal paracentesis is crucial for determining the cause of a patient’s ascites and is indicated for all patients with new onset ascites. Analysis of the ascitic fluid can help determine if the fluid is infected and if it is due to portal hypertension or other causes.
Initial tests that should be performed on the ascitic fluid include: