●The majority of patients with asymptomatic (incidental) gallstones do not require treatment. Patients with symptomatic gallstone disease or those at high risk for developing symptomatic gallstone disease, but are unable or unwilling to undergo cholecystectomy, may be candidates for nonsurgical management.
●Gallstones are composed of a mixture of cholesterol, calcium salts of bilirubinate or palmitate, proteins, and mucin. Based upon the predominant constituents, gallstones are broadly categorized into cholesterol, brown pigment, and black pigment stones.
●Dedicated imaging of the gallbladder is required to evaluate the number and size of stones within the gallbladder and their composition, the patency of the cystic duct, and the concentrating ability of the gallbladder. This can usually be achieved by a combination of computed tomography and oral cholecystography/cholescintigraphy of the gallbladder.
●The goal of nonsurgical management is to reduce the severity of symptoms, clear the gallbladder of stones, and decrease the risk of gallstone related complications. The choice of nonsurgical therapy is based the clinical presentation and stone/gallbladder characteristics as assessed by imaging and patient preferences.
●Ideal candidates for oral bile acid dissolution therapy have all the following characteristics:
•Small stone size (<1 cm)
•Minimal stone calcification and high cholesterol concentration
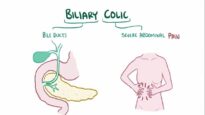
•Mild symptoms of uncomplicated gallstone disease (biliary colic)
•Patent cystic duct
•Good gallbladder mucosal concentration function
●We suggest oral bile acid dissolution therapy with ursodeoxycholic acid (ursodiol) in patients with mild symptoms who have non-calcified small stone(s) in a functioning gallbladder and are not candidates for cholecystectomy (Grade 2B). The decision to use oral bile acid dissolution therapy in symptomatic patients with uncomplicated gallstone disease who are unable/unwilling to undergo cholecystectomy but do not have small noncalcified stones is made on an individual basis taking into account patient preferences.
●We perform an abdominal ultrasound every 6 to 12 months to assess the response to oral dissolution treatment. Ursodiol is continued for at least six months after sonographic clearance of the gallstones. In patients at high surgical/anesthetic risk for cholecystectomy, we continue long-term therapy.
●We reserve percutaneous stone extraction in patients with a cholecystostomy tube either for recurrent symptoms of biliary colic despite oral dissolution treatment or complicated gallstone disease (acute cholecystitis) who cannot undergo surgery. Solitary, radiolucent stones are technically amenable to fragmentation with extracorporeal shock wave lithotripsy (ESWL). However the use of ESWL is limited by high rates of biliary colic and gallstone recurrence after treatment.