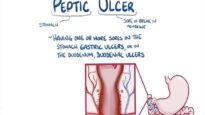
Peptic ulcers are commonly asymptomatic. Symptomatic peptic ulcers most commonly present with epigastric pain or food-provoked epigastric discomfort and fullness, early satiety, and nausea.
Complications
Complications may be heralded by new ulcer symptoms or a change in symptoms, or may occur in the absence of typical symptoms. Complications of peptic ulcers include bleeding, gastric outlet obstruction, penetration into a solid organ or fistulization into a hollow viscus, and free perforation.
Imaging findings
The two direct signs of peptic ulcer disease on abdominal computed tomography scan include focal discontinuity of the mucosal hyperenhancement and luminal outpouching.
Diagnosis
The diagnosis of peptic ulcer disease is suspected in patients with dyspepsia, especially in the setting of nonsteroidal anti-inflammatory drug (NSAID) use or a history of Helicobacter pylori (H. pylori) infection. Occasionally peptic ulcers may be diagnosed or suspected based on contrast imaging performed for evaluation of abdominal pain. The diagnosis of peptic ulcer disease is definitively established by direct visualization of the ulcer on upper endoscopy. On upper endoscopy, benign ulcers have smooth, regular, rounded edges, with a flat, smooth ulcer base often filled with exudate
●Endoscopic features of malignant ulcers
All ulcers with malignant features should be biopsied. Endoscopic features that suggest that an ulcer may be malignant include:
•An ulcerated mass protruding into the lumen
•Folds surrounding the ulcer crater that are nodular, clubbed, fused, or stop short of the ulcer margin
•Overhanging, irregular, or thickened ulcer margins