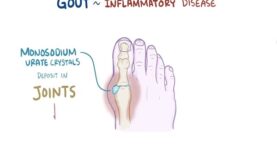
The three clinical stages in the natural history of progressive urate crystal deposition disease (gout) are the gout flare, intercritical (or interval) gout, and chronic gouty arthritis and tophaceous gout. Use of effective urate-lowering therapies has resulted in a reduced frequency of progression of gout to the tophaceous stage. All patients with gout have hyperuricemia (saturation of serum for urate) at some point in their disease, imparting the risk of urate crystal formation and deposition in tissues with inflammatory responses, resulting in the signs and symptoms of gout. Gout flares usually occur after years of asymptomatic hyperuricemia, although most hyperuricemic individuals never experience a clinical event resulting from urate crystal deposition.
Features of gout flares
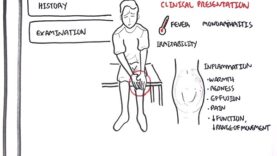
Numerous circumstances promote or are associated with gout flares, which are typically monoarticular and intensely inflammatory, with severe pain, redness, swelling, and disability. Maximal severity of the flare is usually reached within 12 to 24 hours. Complete resolution of the earliest flares almost always occurs within a few days to several weeks, even in untreated individuals. A polyarticular pattern is the initial manifestation in less than 20 percent of patients with gout but occurs with increasing frequency in later flares. Gout sometimes occurs with normal or even low serum urate concentrations at the time of the acute event.
Intercritical gout
Upon resolution of a gout flare, the patient is said to have entered an intercritical (between flares) period, which is most often asymptomatic. This sequence is highly suggestive of the diagnosis. Without urate-lowering treatment, the trend is toward recurrent gout flares that occur after progressively shorter asymptomatic periods and that are increasingly prolonged and disabling, are polyarticular, and may be associated with fever.
Tophaceous gout
Tophaceous gout is characterized by collections of densely packed urate crystals, which are occasionally calcified, in connective tissues and accompanied by a chronic inflammatory response. These collections can be visible and/or palpable but are usually not painful or tender; they can be present on the ears or in the soft tissues, including articular structures, tendons, bursas, or bone. Tophi may be detected with ultrasonography, dual-energy CT (DECT), or MRI. It is likely that many patients with gout and sustained hyperuricemia have a much larger burden of urate crystal deposits than is suspected by clinical examination alone.
Diagnosis
A definitive diagnosis should be sought when a gout flare is suspected, both to exclude alternative explanations for the acute event and to ensure that long-term therapy is not prescribed unnecessarily.
•Crystal visualization
The diagnosis is most secure when supported by visualization of urate crystals by experienced examiners in a sample of fluid aspirated from an affected joint (or bursa). Ultrasonography of joints and adjacent soft tissues is useful for guiding fluid aspiration and can identify specific abnormalities that are highly sensitive and specific for urate crystal deposition. DECT has been standardized and has very good diagnostic yields.
•Use of a “diagnostic” rule
When crystal diagnosis is not achieved, confirmation of the diagnosis of gout can be made in the gout flare setting by use of a “diagnostic rule” utilizing a set of validated clinical, historic, and laboratory criteria.
•Role of findings during intercritical period
During the asymptomatic intercritical period, extracellular urate crystals are identifiable in synovial fluid from previously affected joints in virtually all untreated gouty patients and in approximately 70 percent of those receiving urate-lowering therapy. This allows late establishment of the diagnosis in the majority of patients in whom the diagnosis was not made in the acute setting. Demonstration of urate crystals in aspirates of tophaceous deposits provides a convenient and specific means to corroborate the diagnosis in gouty individuals with clinically detectable tophi.
●Differential diagnosis
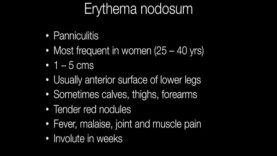
The differential diagnosis of the gout flare includes septic arthritis, trauma, acute calcium pyrophosphate (CPP) crystal arthritis (pseudogout), cellulitis, rheumatoid arthritis, spondyloarthritis, and other types of inflammatory arthritis.