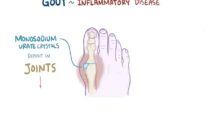
The gout flare is characterized by the presence of monosodium urate (MSU) crystals in synovial fluid obtained from joints or bursas visualized by direct examination of a sample of fluid using compensated polarized light microscop. Urate crystals may also be identified frequently by this technique in material aspirated during the intercritical period from previously affected joints and tophaceous deposits.
The synovial fluid is inflammatory, with white blood cell counts in joint fluid that usually range between 10,000 to 100,000 with neutrophil predominance. Bursal fluid white blood cell counts are usually elevated but to a much lesser degree than joint fluid, similar to findings in patients with septic bursitis.
Blood tests
During a gout flare, blood tests may show nonspecific changes consistent with inflammation; the urate level may be high, normal, or low:
●Neutrophilic leukocytosis and/or elevation of the erythrocyte sedimentation rate (ESR) or C-reactive protein (CRP) are common in gout flares, but their presence in other acute arthritides generally makes these findings of little diagnostic value. An exception to this may be in distinguishing gout from events such as a stress fracture, which may cause some of the above symptoms and physical findings in the absence of laboratory abnormalities and which can be confirmed by imaging studies.
●Serum urate levels can be difficult to interpret during a gout flare. For example, in the early months of urate-lowering drug therapy, gout flares often occur with normal or even low serum urate concentrations at the time of the acute event. Lower urate levels have also been proposed to result from effects of cytokines during flares. Overall, normal to low serum urate values have been noted in 12 to 43 percent of patients with gout flares. In patients suspected of gout based upon clinical features, an elevated serum urate (≥6.8 mg/dL) can lend support to the diagnosis but is thus neither diagnostic nor required to establish the diagnosis. The most accurate time for assessment of serum urate (and establishment of a baseline value) is two weeks or more after a gout flare completely subsides.
IMAGING
Imaging findings consistent with various stages of gout can be seen using several different modalities:
●Plain radiography and magnetic resonance imaging
Subcortical bone cysts apparent on plain radiography or MRI examination can be suggestive of gouty tophi or erosions. Changes of these types seen in imaging procedures are not usually detectable at the time of the first gout flare. More specific gouty lesions, such as delicate “overhanging edges” of bone associated with bone erosions due to tophi, occur with more chronic disease.
The characteristics of tophi on MRI include relatively homogeneous intermediate to low signal intensity on T1-weighted images, as well as on T2-weighted images that have variable signal intensity. Either homogeneous or peripheral enhancement may occur with the addition of gadolinium. These MRI findings, although sometimes supportive of gout, cannot be considered specific, and aspirate confirmation will be needed when the differential diagnosis includes infection or malignancy.
●Ultrasonography
Findings on ultrasound examination can strongly and independently support the diagnosis of gout and may be useful in the early detection and monitoring of therapy. Important diagnostic features include a hyperechoic linear density (double contour sign [DCS]) overlying the surface of joint cartilage or tophaceous-appearing deposits in joints or tendons, which are represented by an ovoid stippled signal (hyperechoic cloudy area [HCA]) surrounded by a hypoechoic border.
A systematic review of the diagnostic performance of ultrasonographic findings in gout found that the DCS had sensitivities and specificities of 83 and 76 percent, respectively. For HCAs consistent with tophus, the estimate was 65 and 80 percent, respectively. A large, multicenter, observational study with concurrent monosodium urate (MSU) validation evaluated the performance of ultrasound features for the diagnosis of gout. The overall sensitivity and specificity of the DCS were 60 and 91 percent, respectively. When comparing those with disease for more and less than two years, only the sensitivity increased meaningfully (from 51 to 63 percent). The overall sensitivity and specificity for HCA consistent with tophus was 46 and 95 percent, respectively. Similar to the DCS, only the sensitivity increased meaningfully (from 34 to 51 percent) when comparing those with disease for less and more than two years.
In patients with asymptomatic hyperuricemia in a small pilot study, both HCA and DCS were found in the joints of some patients who had never had symptoms of gout. The implications of this latter study with regard to making a diagnosis of gout in patients without symptoms of the disease await further discussion and confirmation of the findings.
●Dual-energy computed tomography
Dual-energy CT (DECT) examination can specifically identify urate deposits in articular and periarticular locations and can distinguish urate from calcium deposition. There are potential artifacts with DECT, and ways to minimize them and avoid false-positive interpretations have been described. In a meta-analysis of 13 studies, the pooled sensitivity and specificity of DECT was reported as 89 and 91 percent, respectively. Another study reported an excellent sensitivity for gout of 90 percent but emphasized that all false-negative cases happened in cases with less than six weeks of symptom duration. The yield of both DECT and ultrasound is not expected to vary when a patient is having a flare, as MSU deposition conferring radiologic findings will be present.