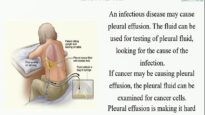
●Thoracentesis is a percutaneous procedure where pleural fluid is removed from the pleural space. It should only be performed by clinicians with experience and who demonstrate competency with the procedure.
●Most patients who have a newly detected pleural effusion should undergo diagnostic thoracentesis. Patients with symptomatic effusions, large effusions, or conditions that risk pleural thickening (eg, tuberculosis, hemothorax) should undergo drainage (therapeutic thoracentesis).
●Contraindications to thoracentesis include insufficient pleural fluid, skin infection or wound at the needle insertion site, and severe bleeding diathesis. Mechanical ventilation with or without positive end-expiratory pressure (PEEP) is not a contraindication to thoracentesis. Decisions to reverse a coagulopathy or correct thrombocytopenia should be individualized and based upon perceived benefits and urgency of thoracentesis versus the probability of bleeding into the pleural space and the ability to tolerate a hemothorax and/or a procedure to drain intrapleural blood, should that be needed.
●Thoracentesis is a sterile procedure that requires informed consent. Several thoracentesis kits are commercially available that contain skin sterilizing fluid (eg, 0.05 percent chlorhexidine), sterile drapes, sterile wound dressing material, local anesthetic, an 18-gauge over-the-needle catheter, stopcock, 35 to 60 mL syringe, and thoracentesis drainage bag/system.
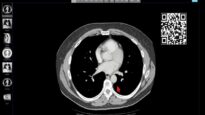
●Thoracenteses should be performed with ultrasound guidance. Before the procedure, the operator rules out pneumothorax with ultrasonography and positively identifies key structures that need to be avoided during needle insertion including the diaphragm with underlying liver or spleen, lung, chest wall, heart, and descending aorta. The procedure is performed immediately following the ultrasonography examination without any patient movement between the time of site selection and needle insertion.
•Ultrasound should guide the selection of the puncture site by identifying an intercostal space with underlying pleural fluid that is of sufficient depth that the lung will not be pierced by the needle during aspiration (typically >10 mm).
•The site is marked with a needle cap, angle and depth of penetration memorized, skin and ribs anesthetized, and fluid removed. In general, 50 mL is sufficient for diagnostic purposes while larger volumes can be removed for therapeutic purposes.
•Following thoracentesis, the ipsilateral chest is examined for pneumothorax by ultrasound. A routine chest radiograph after thoracentesis is not indicated for most asymptomatic, non-ventilated patients, especially if ultrasound suggests that no pneumothorax is present. However, a chest radiograph is indicated if the ultrasound suggests one or is ambiguous, air was aspirated during the procedure, symptoms or signs of pneumothorax develop, ultrasonography imaging was poor, the machine is unable to store images in durable format (ie, for documentation purposes), or multiple needle passes were required. While we typically apply the same practice to ventilated patients, some experts routinely obtain chest radiography in this population.
●Potential complications of thoracentesis include pain at the puncture site, bleeding (eg, hematoma, hemothorax, or hemoperitoneum), pneumothorax, empyema, soft tissue infection, spleen or liver puncture, vasovagal events, seeding the needle tract with tumor, adverse reactions to the anesthetic or topical antiseptic solutions, shortness of breath, cough, and re-expansion pulmonary edema. Pneumothorax, the most common complication that is clinically important, develops in approximately 3 percent of patients or less when ultrasound guidance is used; tube thoracostomy is rarely required for treatment.